Dupuytren Contracture
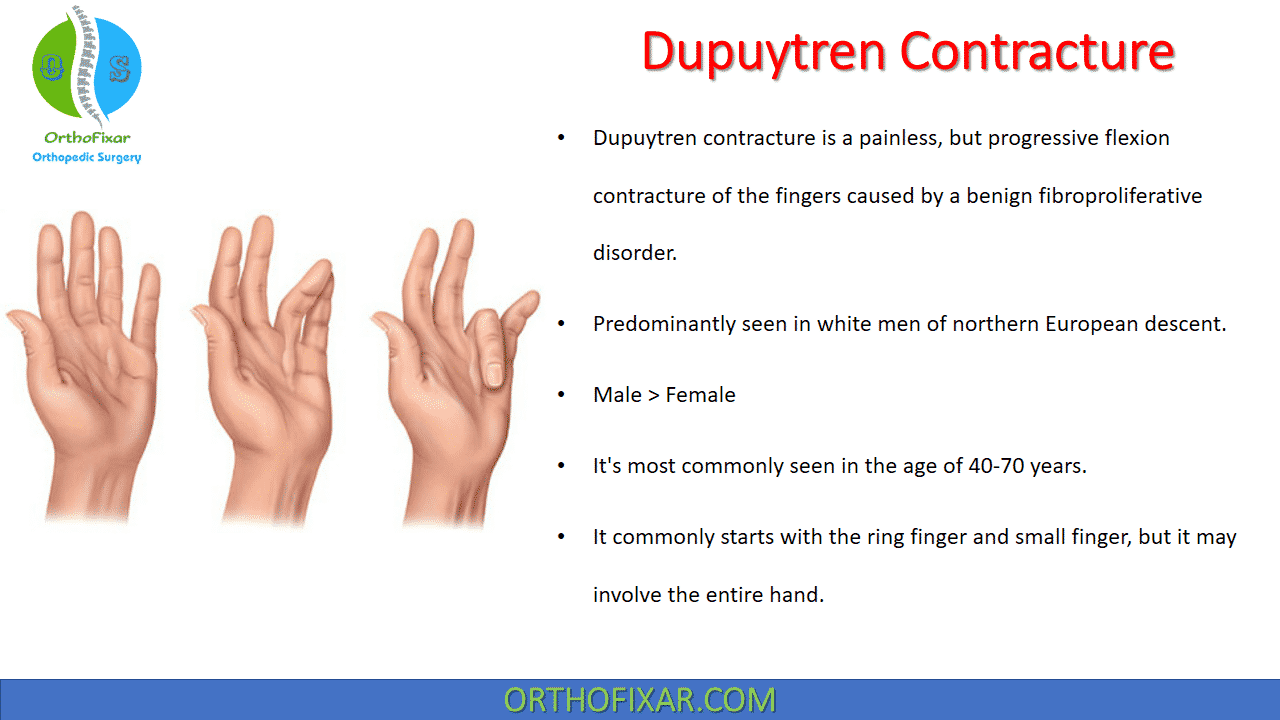
Dupuytren contracture is a painless, but progressive flexion contracture of the fingers caused by a benign fibroproliferative disorder.
It’s historically named as Vikings Disease because this disease originated with the Vikings warriors, who spread it throughout Northern Europe and beyond as they traveled and intermarried. Then it was named after Guillaume Dupuytren , who first described the underlying mechanism of action.
Dupuytren contracture predominantly seen in white men of northern European descent, and Male > Female. It’s most commonly seen in the age of 40-70 years.
It commonly starts with the ring finger and small finger, but it may involve the entire hand. Half of patients have bilateral disease, but this varies with age.
Although an autosomal dominant inheritance pattern with variable penetrance is suspected, the offending gene has not been isolated, and sporadic cases are still more common.
Positive family history is the single strongest predictor of the disease and is associated with both earlier age of onset and earlier age of first treatment. No association with occupation has been determined
See Also: Trigger Finger (Stenosing tenosynovitis)
Related Anatomy
Palm:
The superficial palmar fascia lies in a coronal plane deep beneath the palmar subcutaneous tissue and covers a triangular area of the central palm, the proximal corner facing directly proximal.
The palmaris longus tendon, when present, terminates in continuity with the fibers of this proximal corner. From this common point, four central bands of fascia extend distally toward each of the fingers. There is no central band for the thumb. Confluent proximally, these bands separate and diverge at the distal edge of the underlying transverse retinacular ligament, each following the path of the underlying ray.
At the level of the distal palmar crease, the central bands are bridged transversely by the superficial transverse palmar ligament. At the radial border of the index central band, the superficial transverse palmar ligament is in continuity with the proximal first web-space ligament, which continues to a point roughly superficial to the radial sesamoid of the thumb MCP joint.
Although the superficial transverse palmar ligament appears to lie deep beneath the central bands, fibers from the central bands pass above, below, and through it.
At this level, each central band branches in the following three directions:
- Superficial fibers track superficially to merge with vertical retinacular fibers at the undersurface of the dermis in the distal palm in areas between skin flexion creases, where nodules commonly arise.
- Intermediate fibers split transversely into two sections, which extend toward the lateral border of the base of the digit. This track of fibers is called the spiral band because fibers track around the neurovascular bundle: proximally, they are central and superficial to the bundle; distally, lateral and deep beneath it. Neurovascular spiral bundles result from involvement of these fibers.
- Deep fibers continue dorsally to merge with the sagittally oriented interosseous fascia and pierce the transverse MP ligament to merge with fibers of the sagittal bands of the extensor mechanism. These fibers are rarely involved in contractures.

Web Spaces:
A subdermal fascial layer borders the periphery of the web spaces from thumb to little finger. Fascial fibers follow the direction of this layer. The section of this structure spanning the fingers is referred to as the natatory ligament; its continuation across the first-web space is referred to as the distal first-webspace ligament.
It crosses the thumb to join fibers of the proximal first-web-space ligament over the radial sesamoid area. Fibers from the natatory ligament extend distally at the lateral base of each finger in continuity with the Grayson ligament and the lateral digit dermis.
Digits:
Cleland ligament is dorsal to the neurovascular bundle , and Grayson ligament is palmar to the neurovascular bundle. These “ligaments” are actually a loose meshwork of multiple layers of crossing oblique curved fibers.
There is a common zone of origin of these fibers in continuity with the retinacular ligaments of the fingers, the floor of the flexor tendon sheath, and the network of retinacular fibers that attach to the palmar digital skin.
On the ulnar border of the small finger, this pattern of lateral fascial attachments continues in continuity with the abductor digiti minimi fascia and tendon. What has been described in the digits as the retrovascular band is actually a dissection artifact created by releasing skin attachments of this lateral fascial complex.



Pathophysiology
Dupuytren Contracture has been associated with:
- Tobacco and alcohol use,
- Diabetes,
- Hypercholesterolemia,
- Epilepsy,
- Antiepileptic medication,
- Regional trauma,
- Chronic pulmonary disease,
- Tuberculosis,
- Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS).
- A lower-than-average body mass index.
Myofibroblast contractile properties are abnormal and exaggerated.
There is also increase in ratio of type III to type I collagen and increase in free radical formation.
The Fascial structures that become involved in Dupuytren disease:
- Pretendinous band
- Natatory band
- Spiral band
- Retrovascular band
- Grayson ligament
- Lateral digital sheet
Cleland’s ligament and transverse ligament of the palmar aponeurosis are NOT involved in Dupuytren Contracture.
Dupuytren Contracture Cords:
1. Pretendinous cord:
The pretendinous cord nearly always is responsible for primary contracture of the metacarpophalangeal joint. It may attach to the distal palmar crease skin, base of the proximal phalanx, or the tendon sheath at this level, or it may extend to attach to the flexor tendon sheath over the middle phalanx or the skin in this area.
2. Spiral cord:
A spiral cord occurs when four normally existing structures (pretendinous band, spiral band, lateral digital sheet, and Grayson ligament) become diseased. The spiral cord runs dorsal to the neurovascular bundle proximally and volar to it distally.
When the spiral cord is contracted, the neurovascular bundle is drawn toward the midline of the finger. Neurovascular displacement is found most commonly on the ulnar aspect of the little and ring mfingers, and tedious dissection is required to prevent digital nerve injury
3. Lateral digital cord:
The lateral digital cord may extend distally and contribute to a flexion contracture of the distal interphalangeal joint. The plane between this cord and the overlying skin is minimal and must be developed sharply.
4. Retrovascular cord:
The retrovascular cord is not believed to contribute significantly to flexion contracture of the proximal interphalangeal joint; however, it may be responsible for some residual flexion contracture or recurrence if not excised.
5. Central cord
6. Natatory cord




Dupuytren Contracture Stages
There are three stages of disease described by Luck2 based on histology:
1. Proliferative Stage:
In the proliferative stage, nodules, composed of type III collagen and fibroblasts, develop and expand to displace the subcutaneous tissue and fuse to the skin. The nodules typically appear at the distal palmar crease over the metacarpophalangeal joints and distally over the proximal interphalangeal joints but not over the distal interphalangeal joints. They eventually stop growing and begin to contract in the involutional stage.
2. Involutional Stage:
The nodules stop growing and begin to contract in the involutional stage. Stress alignment of the fibroblasts occurs, and more collagen is produced. Myofibroblasts then replace the fibroblasts as the predominant cell type, producing type III collagen and causing contraction. Nodule contraction places tension on the normal fascia proximally, producing fascial hypertrophy and nodule-cord units.
3. Residual Stage:
In the residual phase, the nodules decrease in size and may become acellular fibrous cords. Contractures of the metacarpophalangeal and proximal interphalangeal joints and displacement of digital neurovascular bundles result from predictable patterns of fascial cord involvement.
Tubiana Staging:
The Tubiana stage is an index of composite flexion contracture. The composite MCP + PIP joint flexion contracture of each ray is placed in a group of 45-degree increments:
- Stage 0: no contracture
- Stage 1: 0 to 45 degrees
- Stage 2: 45 to 90 degrees
- Stage 3: 90 to 135 degrees
- Stage 4: greater than 135 degrees.
DIP joint angles are not included.
See Also: Flexor Tendon Injury of the Hand
Dupuytren Contracture Symptoms
Diagnosis is made by physical examination. there is neither laboratory result, imaging finding, nor a biomarker unique to diagnosis dupuytren contracture.
The earliest signs of Dupuytren Contracture are:
- Skin tightness (exaggerated blanching with finger extension),
- Contour changes (skin crease deformation, dimples),
- Dupuytren Nodules,
- Cords without contractures,
- Prominence of the palmar monticuli.
The earliest appearance of Dupuytren contracture is passive extension deficit due to a contracted cord, most often affecting the MCP and PIP joints of the fingers.
Thumb involvement may result in carpometacarpal (CMC) MCP or IP flexion contractures and/or radial or palmar adduction contractures.
Dupuytren Nodules are flattened round or ovoid areas of subdermal firmness, fixed to the dermis, typically 0.5 to 1.5 cm in diameter with indistinct peripheral margins. The dermal papillae overlying dupuytren nodules may be prominent or may be longitudinally compressed, different from the type of papillary ridge stretching and flattening seen with other slowly growing tumors. Uncommonly, dupuytren nodules are initially erythematous, tender, or itchy. Skin crease deformation or dimples are the first change noticed in about 1 out of 10 patients.
The differential diagnosis of palmar nodules also includes:
- Fibrosarcoma,
- Fibrous histiocytoma,
- Giant cell tumor,
- Synovial sarcoma,
- Calcifying aponeurotic fibroma,
- Epithelioid sarcoma.
Dupuytren diathesis describes patients with early disease onset and rapid progression of joint contractures, often bilateral and including more radial digits
Approximately 5% of patients with Dupuytren contractures have similar lesions in the medial plantar fascia of one or both feet, known as Ledderhose disease, and 3% of patients have plastic penile induration, known as Peyronie disease. Garrod nodules, “knuckle pads” are common on the dorsum of the proximal interphalangeal joints. Patients with these associated findings are considered to have a Dupuytren diathesis and are prone to progressive and recurrent disease.




Dupuytren Contracture Treatment
Nonoperative treatments of Dupuytren Contracture include the following:
1. Range of motion exercises:
Dupuytren Contracture exercises include:
- Finger Lifts: put your finger on the table and hold it up for a few seconds.
- Finger Spreads: put your hand flat on the table and spread all your fingers apart as much as you can and then bring them back together.
- Grip Exercises: try picking up objects or squeeze a small towel or a piece of paper into a small ball.
2. Collagenase injection (derived from Clostridium histolyticum):
Cord is injected directly with enzyme, and patient returns the following day for manipulation of the contracture under digital block anesthesia.
Pooled results of open-label studies demonstrate average MCP correction of up to 85% and PIP correction of up to 60%.
Common adverse effects include temporary pain, swelling and bruising; other complications include skin tears (up to 12%) and flexor tendon rupture (rare).

Operative Treatment:
The indications of surgical treatment of Dupuytren Contracture include:
- Inability to place hand flat on table top (Hueston test).
- MCP flexion contracture greater than 30 degrees.
- Any PIP flexion contracture.
Procedure of choice is typically open limited fasciectomy:
- Iatrogenic digital nerve injury in up to 7% of cases in some series.
- Tourniquet should be deflated prior to closure to assess digital perfusion after large contracture releases.
- Total palmar fasciectomy no longer favored because of high complication rate.

Percutaneous cord release under local anesthetic with a large-gauge needle is an alternative to formal open surgery and may be most favorable in an elderly patient with low demands and multiple comorbidities.
Maneuvers for percutaneous fasciotomy of Dupuytren Contracture :
- A, Anesthetic is limited to the dermis to reduce the chance of a conduction block.
- B, The needle tip is used to clear a working area superficial to the cord.
- C, The needle perforates a line of points across the cord using a reciprocating motion.
- D, The bevel of the needle scores the surface of the cord to progressively divide fibers from superficial to deep.


Open-palm McCash technique with skin healing by secondary intention may still be used to reduce hematoma formation, decrease edema, and allow early motion.
Skin deficits after contracture release may be addressed with Z-plasty, V-Y advancement, full-thickness skin grafting, or healing by secondary intention.
Dupuytren contracture New Treatments
Treatment with microRNA or SiRNA to downregulate the production of TGFβ1 or its receptors, identification of molecules that inhibit or bind to TGFβ1 or other implicated cytokines (the strategy used to develop anti-TNF drugs), and molecular stenting to prevent excessive collagen crosslinking are the types of approaches that must be explored to change the landscape of Dupuytren disease.
Tamoxifen has been shown to reduce recurrence rates after fasciectomy in high risk patients, proof that it is possible to modify Dupuytren contracture biology at first.
Dupuytren contracture Prognosis
The prognosis in Dupuytren contracture seems to depend on the following factors, which may determine the appropriate intervention:
- Heredity: A family history of the disease indicates that the lesion is likely to progress more rapidly than usual, especially if the onset is early.
- Sex: The lesion usually begins later and progresses more slowly in women, who often accommodate better to the resulting deformity; however, long-term results after operation are worse in women than in men, with postoperative flare reaction being twice as likely.
- Epilepsy: Despite earlier statements positively associating Dupuytren contracture with epilepsy, Geoghegan et al. concluded that neither epilepsy nor antiepileptic medications were associated with the disease.
- Diabetes mellitus: Diabetes mellitus is a risk factor for Dupuytren Contracture, especially in patients requiring medical management compared with patients with diet controlled diabetes mellitus.
- Alcoholism or smoking: The lesions are more severe, progress more rapidly, and recur more frequently when associated with these conditions.
- Location and extent of disease: When the disease is bilateral and especially when it is associated with knuckle pads and nodules in the plantar fascia, progression is more rapid, and recurrence is more frequent. Progression is more rapid on the ulnar side of the hand.
- Behavior of disease: How the disease has behaved in the past, whether treated or not, is an indication of its probable behavior in the future.
Complications and postoperative care
- Most common complication after operative treatment is recurrence, with long-term rates as high as 50% (higher in Dupuytren diathesis).
- Early postoperative “flare reactions” are more common in women and may be treated with short courses of oral steroids or NSAIDs.
- Other potential complications include hematoma, infection, digital neurovascular injury, complex regional pain syndrome, and amputation.
Judicious postoperative therapy with active ROM and static nighttime splinting to maintain extension correction is critical for improved outcomes and the prevention or delay of recurrence.
References & More
- Flatt AE. The Vikings and Baron Dupuytren’s disease. Proc (Bayl Univ Med Cent). 2001 Oct;14(4):378-84. doi: 10.1080/08998280.2001.11927791. PMID: 16369649; PMCID: PMC1305903.
- Hart MG, Hooper G. Clinical associations of Dupuytren’s disease. Postgrad Med J. 2005 Jul;81(957):425-8. doi: 10.1136/pgmj.2004.027425. PMID: 15998816; PMCID: PMC1743313.
- LUCK JV. Dupuytren’s contracture; a new concept of the pathogenesis correlated with surgical management. J Bone Joint Surg Am. 1959 Jun;41-A(4):635-64. PMID: 13664703.
- Degreef I, De Smet L. Dupuytren disease: on our way to a cure? Acta Orthop Belg. 2013 Jun;79(3):243-9. PMID: 23926723.
- Campbel’s Operative Orthopaedics 12th edition Book.
- Millers Review of Orthopaedics -7th Edition Book.
- Greens Operative Hand Surgery 7th Edition Book.
March 30, 2023
OrthoFixar
Orthofixar does not endorse any treatments, procedures, products, or physicians referenced herein. This information is provided as an educational service and is not intended to serve as medical advice.
- Lifetime product updates
- Install on one device
- Lifetime product support
- Lifetime product updates
- Install on one device
- Lifetime product support
- Lifetime product updates
- Install on one device
- Lifetime product support
- Lifetime product updates
- Install on one device
- Lifetime product support